Our Technology
 Hexakit researchers are especially focusing on imaging of myocardial infarction (MI) by positron emission tomography (PET). PET is a high-resolution, high-sensitivity nuclear imaging modality which is gaining wider ground in the world of diagnostic medicine.
Hexakit researchers are especially focusing on imaging of myocardial infarction (MI) by positron emission tomography (PET). PET is a high-resolution, high-sensitivity nuclear imaging modality which is gaining wider ground in the world of diagnostic medicine.
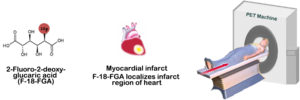
Current techniques of imaging MI are based on detection of tissue viability by lack of perfusion in the infarcted region. Novel PET agent F-18-labeled fluoroglucaric acid (F-18-FGA), which is being investigated in pre-clinical models, does not depend on perfusion defect to detect MI. On the contrary, F-18-FGA accumulates in acute infarct to positively delineate the presence of necrotic tissue.
Innovation
F-18-FGA demonstrates diagnostic potential in the early detection of acute MI because of its early myocardial distribution and rapid blood-pool clearance. It can help discriminate necrotic regions from ischemic segments, which is not possible by perfusion imaging alone.
F-18-FGA is the first patent-pending product for infarct imaging by PET which enables high resolution imaging of MI. F-18-FGA undergoes rapid clearance and does not accumulate in the liver or lungs which would otherwise create imaging artifacts. SPECT perfusion agents suffer from this problem of extra-cardiac accumulation.
F-18-FGA targets cellular changes that occur early in MI. Thus, it can diagnose MI, even in patients with normal ECG (non-STEMI) and ambiguous troponin levels.
F-18-FGA can be easily produced in nuclear pharmacies, medical cyclotron facilities, or in nuclear cardiology labs using a kit and commercially available F-18-FDG. This ease of synthesis eliminates the need to deviate cyclotron production cycles towards synthesis of a specialized product, which reduces the cost of an F-18-FGA dose.
Impact
According to a report from the American Heart Association, about 735,000 Americans suffer an MI every year, of which approximately 20% are silent MI- the damage is done, but the person is not aware of it. Early and definitive diagnosis of acute MI is necessary to initiate therapy to salvage myocardium at risk and to avoid unnecessary course of treatment. The short time-window available for effective thrombolytic therapy necessitates that the results of diagnosis are available quickly.
F-18-FGA/PET is predicted to eliminate the possibility of missed MI diagnosis by providing information about the location and extent of infarct. While infarct imaging with F-18-FGA/PET will be most impactful in the detection of acute myocardial infarction, its combination with perfusion information will assist in assigning treatment course involving medical therapy or revascularization. For instance, it is important to discern which patients will respond to the risky, invasive, and expensive procedure of revascularization. Identification of irreversibly damaged tissue will aid in optimal allocation of treatment, sparing patients who might not benefit from revascularization. Approximately 18% of revascularized patients fall into this category. Post-revascularization, F-18-FGA/PET will be highly useful in assessing the revascularization success. Further indications for F-18-FGA/PET are myocarditis and cardiac transplant patients for evidence of rejection.